|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 2
| Issue : 1 | Page : 25-30 |
|
Techniques in the removal of impacted mandibular third molar: A comparative study
Vibha Singh, Khonsao Alex, R Pradhan, Shadab Mohammad, Nimisha Singh
Department of Oral and Maxillofacial Surgery, K.G.M.U. Lucknow, Uttar Pradesh, India
| Date of Web Publication | 2-Feb-2013 |
Correspondence Address:
Vibha Singh
A 43 Krishna Nagar, Lucknow, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2278-9626.106799

Objective: Surgical removal of impacted third molar is one of the common surgical procedures carried out in Oral and Maxillofacial Surgery set up. This study aimed at clinically assessing the three different surgical techniques (lingual split, using chisel and mallet, buccal approach techniques, using rotary instruments used in the removal of impacted mandibular third molars. Materials and Methods: The present clinical study comprised of 150 impacted mandibular wisdom teeth. Patients were divided in three groups and bone covering the third molar was removed by the Lingual split technique using chisel and mallet, Buccal approach technique using chisel and mallet, and Buccal approach technique using rotary instruments. Results: Surgical time was significantly increased in bur technique. Trismus was significantly increased in lingual split technique and bur technique from buccal approach technique using chisel and mallet. Post-operative nerve injury was significantly higher in lingual split technique. Dry socket was more in patients of bur technique. Conclusion: In this study we found that lingual split technique using chisel and mallet is found to be better among all three techniques used followed by buccal approach using chisel and mallet and the buccal approach technique using rotary instruments. Keywords: Lingual split technique, paresthesia, trismus
How to cite this article:
Singh V, Alex K, Pradhan R, Mohammad S, Singh N. Techniques in the removal of impacted mandibular third molar: A comparative study. Eur J Gen Dent 2013;2:25-30 |
How to cite this URL:
Singh V, Alex K, Pradhan R, Mohammad S, Singh N. Techniques in the removal of impacted mandibular third molar: A comparative study. Eur J Gen Dent [serial online] 2013 [cited 2021 May 10];2:25-30. Available from: https://www.ejgd.org/text.asp?2013/2/1/25/106799 |
| Introduction | |  |
Surgical removal of impacted third molar is one of the common surgical procedures carried out in the oral and maxillofacial surgery set up.
Surgical management of impacted third molar is difficult because of its anatomical position, poor accessibility, and potential injuries to the surrounding vital structures, nerves, vessels soft tissues, and adjacent teeth during surgeries.
The factors contributing to the post-operative morbidity are many, but the most important one is the trauma from bone cutting as the procedure involve significant bone cutting, which is carried out either by chisel and mallet or by rotary cutting instruments (like surgical bur).
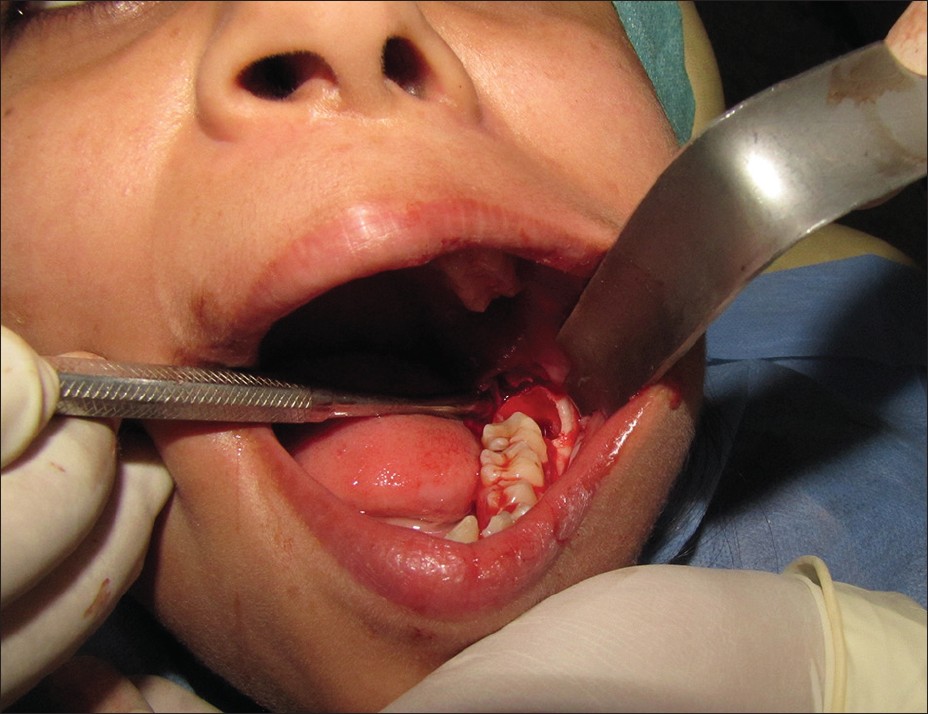
This study aimed at clinically assessing the three different surgical techniques (lingual split, using chisel and mallet, buccal approach techniques, using rotary instruments used in the removal of impacted mandibular third molars as regards their convenience, time taken, post-operative sequel/complications) [Figure 1], [Figure 2] and [Figure 3].
| Materials and Methods | | |
The present clinical study comprised of 150 impacted mandibular wisdom teeth. A thorough history of all cases was recorded, and clinical examination was carried out. Patients having debilitating diseases were not included in this study. Routine blood investigations were done in all the patients and specific investigation whenever required. Intra-oral periapical radiograph and orthopantomograph was done whenever required.
The patients were divided in three groups irrespective of cast, creed, age, sex, and social economic status. Pre-and post-operative recording were made on the format designed for the study. All the patients were pre-medicated with ciprofloxacin 500 mg + tinidazole 600 mg BID dose, and chlohexidine mouthwash starting two days before surgery 3-4 times daily. All the patients were operated under local anesthesia inferior alveolar, and long buccal nerve blocks were given to achieve desired local anesthetic effect.
A standard incision (Wards's incision) [1] was made in all cases. The tissue flap was reflected buccally, distally, and legally to expose the tooth and bone. Wide end of Hawarth's elevator was inserted in the lingual plate marginal to third molar and overlying mucosa and held close to the bone to protect lingual nerve.
Bone covering the third molar was removed by the,
- Lingual split technique using chisel and mallet,
- Buccal approach technique using chisel and mallet,
- Buccal approach technique using rotary instruments.
Lingual split technique using chisel and mallet. Given by Sir William Kelseyfry, published by T.G. Ward (1956)
First, a vertical stop cut was made distal to second molar using 3 mm chisel bevel end facing towards the second molar, which will prevent splitting of the bone along the buccal aspect of second molar, greater the depth of the wisdom tooth, longer the stop cut was made. After establishing the point of elevation, the distal bone was removed to allow the delivery of the tooth. To remove this piece of bone, a 5 mm chisel was placed distal to the third molar with the beveled side upward and cutting edge parallel to the external oblique ridge. The chisel was driven to the depth required, which varies with the depth of the wisdom teeth and when desired level is reached, the chisel is removed and replaced with the beveled side down wards. Thus, the direction of the cut is altered from downwards to inwards towards the lingual plate without alteration in the direction of the chisel. When the bone is split, the chisel is twisted further and lingual plates breaks anteriorly at its thinnest point, this is where the crown of the third molar is nearest to the lingual surface. Then, the lingual splitted bone is removed, and the entire distolingual aspect of the impacted tooth is exposed.
Buccal approach technique using chisel and mallet
First, a vertical stop cut was made distal to second molar using 3 mm chisel bevel end facing towards the second molar, which will prevent splitting of the bone along the buccal aspect of second molar, greater the depth of the wisdom tooth, longer the stop cut was made. After establishing the point of elevation, the distal bone was removed to allow the delivery of the tooth. To remove this piece of bone, a 5 mm chisel was placed distal to the third molar with the beveled side upward and cutting edge parallel to the external oblique ridge.
In this case, lingual plate was not removed, but the point of application of elevator and direction of force of elevation is same as lingual split technique.
Buccal approach technique using rotary instruments
Rose head round bur/straight fissure bur were mounted on a low speed micrometer straight hand piece to remove the bone. A vertical cut was made using straight fissure bur with the same principal using saline as coolant. The point of application of elevation is same as other technique described.
After removal of impacted third molar, wound was inspected carefully and checked for bone piece tooth follicles granulation tissues. Suturing was done by using 3-0 black silk. Same antibiotics and analgesic was given to all patients. Total surgical time was noted (Incision-making till the last suturing was finished).
Evaluation of the procedure
Evaluation was done on a format, in which following parameters were taken
Intra-operative
Operative time taken, breakage of root, injuries to adjacent teeth, fracture mandible, displacement of tooth in sublingual space, injury to soft tissue and tongue.
Post-operative
Hemorrhage
Bleeding was observed periodically at the interval of 10, 30, and 60 minutes. This was done through visual inspection on the pack given after surgery and expressed in terms of scanty, moderate, and severe.
Pain
Seymour [2] visual pain scale
Numerical scale

Swelling
Post-operative swelling was recorded using Breytenbach [3] method of measurement tragus to pogonion (ear to chin) comparison between pre- and post-operative measurement.
0 = no swelling
1 = mild swelling
2 = moderate swelling
3 = severe swelling.
Trismus
It is most objective finding; it was measured by measuring inter-incisal distance.
Infection
Nerve injury
0 = no sensational impairment
1 = mild loss of sensation
2 = moderate loss of sensation
3 = severe loss of sensation
Dry socket
All post-operative patients' follow-up was done on day 1 st , 3 rd , and 5 th post-operative day. Comparison of result was done up to 5 th post-operative day. The patients with persistent problems were continued 10 th , 20 th , and 30 th post-operative day.
| Results | | |
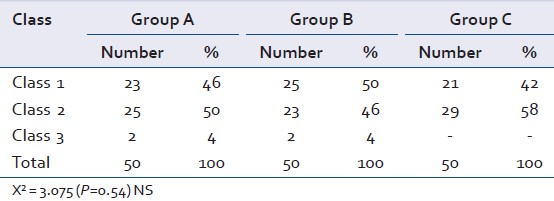
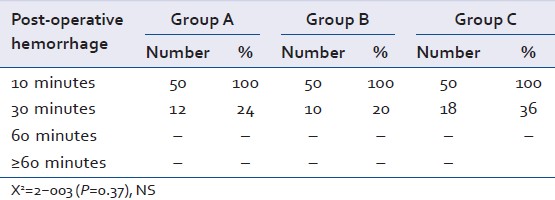
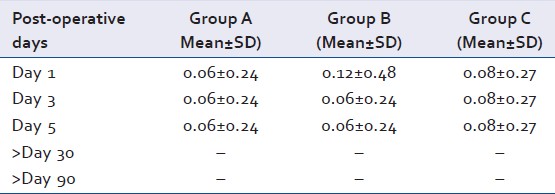
The study was comprised of 150 patients who were randomly divided in three groups according to surgical technique employed to them, each group comprising of 50 patients [Table 1]. Class-wise distribution of impacted teeth taken in the study was similar [Table 2]. Surgical time was significantly increased in group C followed by group B and minimum in group A [Table 3]. Displacement of tooth in the sublingual space was found in only 1 patient of group A [Table 4]. Post-operative hemorrhage was similar in all the groups, and within 10 minutes, there was no significant difference among these groups [Table 5]. There is significant reduction in post-operative swelling at post-operative day 3 and post-operative day 5 among groups A, B, and C [Table 6]. Trismus is significantly increased in group A and group C from group B (Trismus was measured using Wood and Branco [4] method measuring inter-incisal distance by graduated ruler and expressed in cm) [Table 7]. Pain score decreases significantly with time. It is maximum at day 1 and minimum at >5 in each groups. In groups, pain was maximum in group A than in group C and in group B [Table 8]. Post-operative nerve injury is significantly higher in group A than in group B and C. It decreases significantly after day 5 in each group [Table 9]. Dry socket was more in patients of group C than in group A and B [Table 10].
| Discussion | | |
Many problems associated with the removal of mandibular third molar impaction have led us to compare the prevalent technique for their efficacy. The present study was undertaken to assess clinically the level of effectiveness of three different bone cutting techniques and approaches to remove investing bone in the removal of impacted mandibular wisdom teeth.
In this study, asymptomatic patients were included and randomly grouped in three groups as follows:
Bone covering the third molar was removed by the,
- Lingual split technique using chisel and mallet,
- Buccal approach technique using chisel and mallet,
- Buccal approach technique using rotary instruments.
Same pre-medication were given to all patients, and same regime of antibiotic analgesic was prescribed.
Authors [5] using lingual split and Thoma [6] and Archer [7] using buccal bone cutting mentioned that swelling was a known complication of third molar surgery. The presence of swelling or infection causes spasm of muscle leading to trismus. Bleeding can be attributed to two factors primarily due to dislodgment of clot and secondary due to infection. [6],[7],[8]
Surgical time depends on various factors like patient's co-operation, instruments used, experience of the surgeon, and surgical accessibility from patients to patients. Most of the patients in the study were operated in between 30-60 minutes. Most of the patients in the study were operated between 20-30 minutes [Table 3]. The study shows that group C took maximum time; the reason may be bone cutting with bur at low speed and suctioning the coolant, more assistance, and seldom used technique in this institute. The minimum time taken in the group was group A; the reason in the favor of this technique which has been in since many years at this center.
Displacement of tooth was found only in one case, which was in group A [Table 4]. In our study observation, the reason might be used of a blunt instrument, which fractured the lingual cortical plate more than expected unguided elevation and position of the tooth in the bone, which was in position C.
Post-operative hemorrhage was similar in all three groups [Table 5]. Within 10 minutes, there was no significant change in groups. At 30 minutes, percentage was slightly higher in group C than in group A and was maximum in group B, but non-significant.
Post-operative swelling we used Breytenbach [3] method measurement from tragus to progonion (ear to chin) there is significant reduction in post-operative swelling at day 3 and day 5 among the group A, B, and C.
Swelling was maximum in group C than in group B and was minimum in group A; reason for more swelling in group C may be that electric-driven instruments generates a certain amount of onwards transmission force enough to drive the bone particles deeper to bony canaliculi; another reason may be inability to achieve complete sterilization of bur and hand piece assembly, which lead to cross-infection and brushing of surrounding tissues. [8]
Trismus
In this study, trismus score was found significantly higher in group A and C than in group B. Our finding is similar to Rud [9] finding where trismus was higher in lingual split technique. The reason might be due to overstressing of lingual retractor to lingual oral mucosa bruising of surrounding muscles, mylohyoid muscles, medial pterygoid muscle, part of thick tendon of temporalis muscle by retractor, chisel, and lingual cortical bone piece are the added factors for the trismus.
Pain decreased significantly with time. It was maximum on post-operative day 1 and minimum at day 5. In our study, significant difference was not found in different groups.
Kruger [5] and Thoma [6] have mentioned pain to be post-operative complication in third molar surgery while using buccal approach.
Post-operative nerve injury impairment of sensation [Table 9] was found maximum in group A followed by group B and was minimum in group C. Impairment of sensation in all groups were temporary lasting from 1 week to 3 weeks only. Von Arc [10] reported high incidence of lingual nerve injury (22%), which was similar to our finding in group A.
In group B, our finding corroborates with the finding of Rood [11] inferior alveolar nerve injury to be 12.07% temporary. Von Arc [10] reported inferior alveolar nerve injury (5%), which is slightly less than our finding in group C. Our finding of lingual nerve injury in group A cannot be taken as conclusive result, because surgeries were performed by many surgeons including PG trainee with the changing assistance.
Post-operative dry socket was maximum in group C [Table 10] followed by group A and was minimum in group B.
Birn, [12] MacGragor [13] reported 5-10% incidence of dry socket, which is similar to our findings, and overall incidence of dry socket was 12% in our study. Simpson stated that if bur or chisel were used correctly, post-operative recovery was almost similar.
Lilly [14] and Horton [15] showed that results were better while using bur.
Szmyd et al.[8] evaluated the high speed bur technique verses chisel mallet clinically and found no significant difference in post-operative swelling, trismus, and pain and other symptoms, which does not support our study.
From the above study, we infer that there are various advantage in lingual split technique like less operative time, less hemorrhage, less swelling, less infection, and less incidence of dry socket as compared to two other techniques.
| Conclusions | | |
The assessment of effectiveness of three surgical techniques in the removal of impacted mandibular teeth was made on the basis of ease of surgical technique and different post-operative findings. Clinical impression made in each technique were as follows: There was no significant difference in post-operative hemorrhage, there was difference in total surgical time taken, it was found that surgical time was significantly minimum in lingual technique using chisel and mallet.
Post-operative swelling and pain were more in buccal approach using rotary instrument followed by buccal approach using chisel and mallet and minimum in lingual split technique.
Incidence of dry socket was significantly higher in buccal approach using burs in comparison to other groups. Temporary paresthesia and trismus were not significant in two groups, but in lingual technique, there was marked increase in temporary neurological disturbance for two to three weeks and trismus for one or two weeks.
Lingual split technique using chisel and mallet is found to be better than other two groups.
| References | | |
| 1. | Ward TG. Split bone technique for removal of lower third molar. Br Dent J 1956;101:297-301. 
|
| 2. | Seymour RA. The use of pain scales in assessing the effect of analgesics in post operative dental pain. Eur J Clin Pharmacol 1982;23:5441-4.
[PUBMED] |
| 3. | Breytenbach HS. Objective measurement of post operative swelling. Int J Oral Surg 1978;7:386-92.
[PUBMED] |
| 4. | Wood GD, Branco JA. A comparison of three methods of measuring maximal opening of the mouth. J Oral Surg 1979;37:175-7.
[PUBMED] |
| 5. | Textbook of Oral and Maxillofacial Surgery. Kurger GO, editor. 6 th ed. Mosby: New Delhi: Jaypee Brothers; 1990.
|
| 6. | Thoma KH. Oral Surg. In: Bioanatomy. 4 th ed, Vol. 1. St Louis: C. V. Mosby Co.; 1963. p. 29.
|
| 7. | Archer WH. Oral and Maxillofacial Surgery. 5 th ed, Vol. 1. USA: W.B. Saunders Company; 1976.
|
| 8. | Szmyd L, Hester WR. Crevicular depth of the second molar in impacted third molar surgery. J Oral Surg 1963;21:185-9.
[PUBMED] |
| 9. | Rud J. The split-bone technique for removal of impacted mandibular third molars. J Oral Surg 1970;28:416-21.
[PUBMED] |
| 10. | Von Arx DP, Simpson MT. The effect of dexamethasone on neuropaxia following third molar surgery. Br J Oral Maxillofac Surg 1989;27:477-80.
[PUBMED] |
| 11. | Rood JP. Degree of injury to the inferior alveolar nerve sustained during the removal of impacted mandibular third molars by lingual split technique. Br J Oral Surg 1983;21:103-16.
[PUBMED] |
| 12. | Brin H. Etiology and pathogenesis of fibrinolytic alveolitis (dry socket). Int J Oral Surg 1973;2:211-63.
|
| 13. | MacGregor AJ, Addy A. Value of penicillin in the prevention of pain, swelling and trismus following the removal of ectopic third molars. Int J Oral Surg 1980;9:166-72.
[PUBMED] |
| 14. | Lilly GE, Osborn DB, Rael EM, Samuel HS, Jones JC. Alveolar Osteotis associated with mandibular third molar extraction. J Am Dent Assoc 1974;88:802-6.
|
| 15. | Horton JE, Tarpley TM Jr, Jacoway JR. Clinical applications of ultrasonic instrumentation in the surgery removal of bone. Oral Surg Oral Med Oral Pathol 1981;51:236-42.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7], [Table 8], [Table 9], [Table 10]
| This article has been cited by | | 1 |
A Unique Way of Removing Mandibular Third Molars - Implosion Technique |
|
| Mohmed Isaqali Karobari,Jawaad Ahmed Asif,Tahir Yusuf Noorani | | Journal of Evolution of Medical and Dental Sciences. 2021; 10(10): 752 | | [Pubmed] | [DOI] | | | 2 |
Efficacy of sticky bone as a novel autologous graft for mandibular third molar extraction socket healing - An evaluative study |
|
| TaherAbbas Rupawala,ShitalMayank Patel,NaiyaHitesh Shah,KunjBhupeshchandra Sanghvi,SanjayVinubhai Makwana,KrunaKantilal Bhimani | | Annals of Maxillofacial Surgery. 2020; 10(2): 335 | | [Pubmed] | [DOI] | | | 3 |
Comparison of intrasocket bupivacaine administration versus oral mefenamic acid capsule for postoperative pain management following removal of impacted mandibular third molars |
|
| Ideh Talimkhani,Mohammad Reza Jamalpour,Hamed Babaei,Javad Faradmal | | Journal of Oral and Maxillofacial Surgery. 2019; | | [Pubmed] | [DOI] | | | 4 |
A pilot study on the effects of direct contact of two different surgical burs on the cadaveric lingual nerve |
|
| S.M. Al-Amery,W.C. Ngeow,P. Nambiar,M. Naidu | | International Journal of Oral and Maxillofacial Surgery. 2018; | | [Pubmed] | [DOI] | | | 5 |
Associations between dental anxiety and postoperative pain following extraction of horizontally impacted wisdom teeth |
|
| Tze-Fang Wang,Ya-Ting Wu,Chien-Fu Tseng,Chyuan Chou | | Medicine. 2017; 96(47): e8665 | | [Pubmed] | [DOI] | | | 6 |
Comparison of the efficacy and safety of 2% lidocaine HCl with different epinephrine concentration for local anesthesia in participants undergoing surgical extraction of impacted mandibular third molars |
|
| Myong-Hwan Karm,Fiona Daye Park,Moonkyu Kang,Hyun Jeong Kim,Jeong Wan Kang,Seungoh Kim,Yong-Deok Kim,Cheul-Hong Kim,Kwang-Suk Seo,Kyung-Hwan Kwon,Chul-Hwan Kim,Jung-Woo Lee,Sung-Woon Hong,Mi Hyoung Lim,Seung Kwan Nam,Jae Min Cho | | Medicine. 2017; 96(21): e6753 | | [Pubmed] | [DOI] | | | 7 |
Extraoral Surgical Approach of Ectopic Mandibular Third Molar to the Lower Border of Mandible |
|
| Luigi Laino,Dardo Menditti,Lorenzo Lo Muzio,Gregorio Laino,Floriana Lauritano,Marco Cicciù | | Journal of Craniofacial Surgery. 2015; 26(3): e256 | | [Pubmed] | [DOI] | |
|




 |
|
|
|




 Search Pubmed for
Search Pubmed for